
Interested in rare diseases? Here are some facts in acknowledgement of #RareDiseaseDay 2016
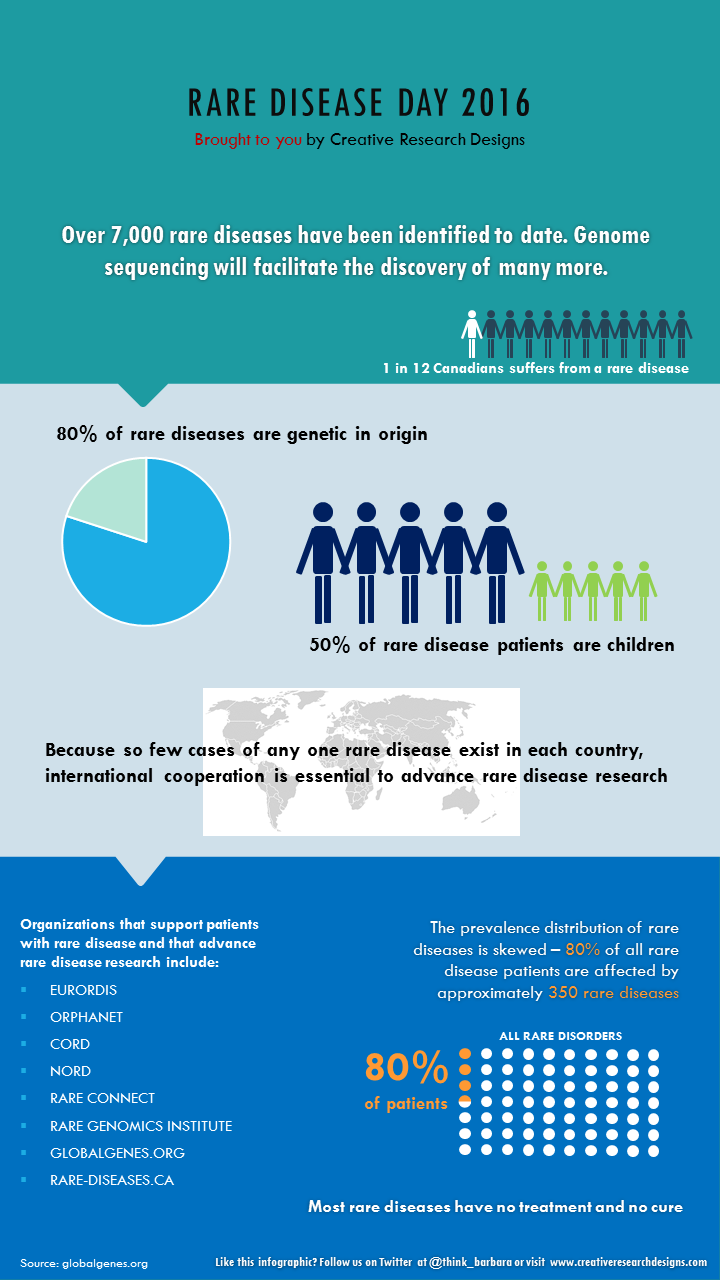
Interested in rare diseases? Here are some facts in acknowledgement of #RareDiseaseDay 2016
Healthcare is going digital at a rapid pace. A recent article by McKinsey & Company titled ‘How pharma can win in a digital world’ outlines emerging trends in digital health and how pharma needs to evolve to keep up with the times.
A number of predictions in this article are, I believe, misguided and reflect a common, but incorrect understanding of the potential of digital in health.

Prediction # 1: “Patients are becoming more than just passive recipients of therapies”
Patients have certainly become more knowledgeable about their own health and about available therapies. And hopefully, health-related apps are helping people lead a healthier lifestyle and stay on top of their medical conditions and medications. However, patients have never been passive recipients of therapies. Patients have always had the choice of taking or not taking their pill, cutting it in half, skipping a dose, forgetting to take it, taking it with food when they are not supposed to etc.
Having served pharmaceutical clients for more than a decade, I have frequently observed that it is difficult for someone within the industry to understand that the medicine they are producing is not the be-all and end-all of a patient’s existence. Life is a busy thing. You work, you look after your family, you eat, you entertain yourself, and you may have a health problem that benefits from taking a medication. The act of taking a pill consumes a fraction of your time and attention. Medicines for health issues that are non-symptomatic may be forgotten because the patient does not feel sick. Medicines for chronic, life-threatening conditions may have suboptimal compliance because the patient would rather not be constantly reminded about his or her precarious situation. For acute conditions, compliance wanes as soon as the patient feels better. Side effects deter patients from taking their pill, etc. Compliance would not be such a huge unsolved problem for pharma if patients were ‘passive recipients of therapies’.
Prediction # 2: “Patients will be actively designing the therapeutic and treatment approaches for themselves with their physicians”
I have read this type of statement numerous times in articles about the future of pharma. Perhaps I am lacking understanding of what’s technologically possible nowadays, but for now let’s assume I have a pretty good handle on it. Designing a pharmaceutical product is an extremely specialized and complex process that involves scientists and labs. A chemical or biological compound with certain properties is created to address a specific health issue, and this compound cannot be easily customized. Rather, it is created and then subjected to rigorous testing, costing hundreds of thousands of dollars (or more), and if it does not hold up to scrutiny, then it’s back to the lab for more experiments and tweaking before another round of expensive testing resumes.
Physicians who spend most of their time in clinical practice do not design therapeutic and treatment approaches. They are merely the retailers of those approaches, acting as consultants to their patients and advising them which approach may be best suited for them. And patients will not be actively designing their own therapies unless they are experimenting with mixing pills and brewing up concoctions of their own invention (caution: don’t try this at home, kids!).
With substantially increased access to information patients can play a much more active role in selecting treatments, but they will not design them.
Prediction # 3: “Medicine will be personalized to address individual patients’ needs” (not in McKinsey article, but can be found in many other publications on digital health).
The move towards personalized medicine is certainly well underway. However, it does not mean that a therapy will be designed on the spot for the individual sitting in front of his or her physician. Again, the physician is the expert mechanic using existing wrenches and bolts to fix the car. The inventor who comes up with new wrenches and bolts does not deal directly with the customer whose car broke down.

Personalized medicines are medicines that target issues more precisely than was previously possible. While physicians used to set off a grenade to blast away your breast cancer, and half of your body as well, they now use a precision rifle that locks in on the malignant area and eliminates not much else. And depending on your genetic profile, there are different bullets that are most effective for your particular type of problem. So the array and precision of weaponry in the physician’s arsenal has increased vastly, and affordable genetic tests have contributed to better targeting of the weapons. But none of these things are designed on the spot, while you’re sitting in the examining room, nor will this be possible for a long, long time.
Explanation: Poor understanding of digital vs. physical contributes to common misperceptions
How do these misconceptions come about and why do smart people write these things?
The past five to ten years of our experience of living in a digital world have greatly impacted our beliefs in how easily things can get done and our feeling of agency. Want to customize your new car? Just click on the features that you want – sunroof, heated seats and the colour red – and you can get this exact model without any effort on your part. Select the perfect outfit? Choose the style, colour and size, and get it delivered to your doorstep the next day. Don’t like part of your video? Just delete and replace.
The ease of these digital experiences has gotten us into the mindset that things can be designed instantaneously, delivered rapidly and modified on the spot. We rarely think about the physical realities that enable our digital experiences. To give you the experience of ‘designing’ the perfect outfit for yourself, the maker has to come up with new styles to attract your desire, run efficient manufacturing to put the piece together with acceptable quality and at an affordable price, ensure the supply chain to enable the manufacturing, build in agility to adapt supply to demand quickly, and create a distribution system to bring the piece to you. All of these things are not done through click of a button, but through the hard work of setting up systems, negotiating agreements, fine-tuning machinery and materials and implementing physical processes.
It’s the same for pharmaceutical products. They are chemical compounds, after all.
Digital opportunities
However, the potential of digital solutions to transform the way we care for ourselves and the way healthcare is provided to us is undisputed. From life tracker apps that help you remember to take your pills on time to smart contact lenses that monitor blood glucose levels without pricking your finger to ingestible sensors that give you peace of mind that your schizophrenic brother has actually taken his medication, digital interfaces, algorithms and sensors can deliver great value to the patient.
The question is how this translates into business opportunities. Many people believe that pharmaceutical companies should transform themselves from being “a products-and-pills company to a solutions company” (see McKinsey & Company article). The idea is to not only provide medicine to the patient but also digital tools for monitoring of the patient’s condition, for communicating with the patient’s circle of care, for scheduling and reminders, for supporting rehabilitation after events and for outcomes tracking. From a patient perspective, this could certainly be a valuable offering. From a business perspective, the value proposition is less clear.
First of all, pharma companies do not typically have the expertise to develop digital solutions in house. Some form alliances with tech companies. Novartis and Google are developing smart contact lenses for people with diabetes and are scheduled to start trials this year. Otsuka and Proteus Digital Health have teamed up to embed a digital sensor into a schizophrenia medication to track compliance, and have submitted the first digitally enhanced new drug application to the FDA. J&J has set up a series of incubators and rewards startups for coming up with interesting ideas in digital health. Merck sponsors health hackathons.
What does the pharmaceutical company get out of this? Will physicians choose their medication over competitive products because it comes with a digital value add? Is the digital component just another cost factor that is necessary to stay competitive these days, or is there a revenue model somewhere? It seems that there is currently a climate of experimentation without a clear business model path ahead, not unlike many other areas of digital development.
In crowded markets with little product differentiation, it is possible that the companion app could become the deciding factor in recommending one drug over the other. However, it is hard to imagine that it would play any role if there were differences in efficacy or side effect profile between the compounds. A tricky little question is also what to do with patients who need to switch off one product and go to another. Should they be denied continued usage of the app?
To be truly solutions providers, pharma companies would need to be structured differently, around disease states, not around products. It would make more sense to form a company that is, say, a ‘cardiology broker’, offered great digital tools to manage a variety of cardiologic conditions and give patients access to the full gamut of cardiology drugs available. The sales reps for this company would not overtly or covertly ‘push’ one or two drugs, but they would advise physicians on what is new in the field and impartially discuss the merits of the different options. There are some attempts of pharma companies to become leaders in a therapeutic space and assume the role of expert provider – for example Roche or Novartis in oncology, where both companies have a large product portfolio. However, by and large, this type of business model does not apply to how pharma companies are organized and how they make money currently. It would be more applicable to private payors, and we see some organizations in the U.S. moving in this direction.
Low-hanging but sour fruit
The obvious area where digital tools can be used very effectively to drive engagement is patient-related. Arguably, a more engaged patient will likely be more compliant and stay on therapy longer, resulting in immediate benefit to the bottom line.
However, while many companies try to be patient-centric, any direct engagement with a patient carries the risk of an adverse event report with it. While adverse event reporting systems have been set up to keep patients from harm, unfortunately, reporting requirements are ridiculously broad. Nobody is keen on generating massive amounts of adverse event reports for their drugs. So digital engagement of patients has to be done with all sorts of caveats to reduce the risk of learning about an adverse event. Some companies stay away from direct engagement with patients altogether for that reason; others have taken the plunge and struggle to come up with creative ways around the problem.
Another challenge in engaging with patients through digital tools and platforms is finding appropriate engagement formats for particular audiences. A platform that has been designed to help kids with pain through gamified challenges and ‘levels’ may not be the right approach to engage a 70-year old cancer patient. Very little testing and research has been done to date to find out what tools best support patients with certain conditions. The key here is to be open to a multi-platform approach. While a game may be great at motivating one audience, a combination of text reminders and phone support may be best suited to keep another audience adherent to their treatment. Unfortunately, many of the vendors that design patient engagement tools on behalf of pharma are either all digital or not digital at all. What would be needed is a new type of vendor who can pull together various types of tools and customize them for a particular target patient population.
Low-hanging sweet, sweet fruit
One area where pharma could employ digital innovation easily and with sustained impact is in the way companies communicate with physicians. While almost everyone has switched to iPads for detailing over the past few years, pharma companies (in Canada, my home turf) still have limited understanding of how digital can be used to improve access and deliver value to physicians. Knowledge about different forms of digital engagement is lacking in marketing departments where people think Twitter and Instagram are for self-absorbed teenagers with too much time on their hands. Also, there is a feeling that digital is not important to the physicians who are core to the business. However, as one year after another go by and younger physicians become key opinion leaders and high prescribers, companies may find that they have missed the boat in establishing a digital rapport with these individuals.
Only recently have some companies started to think about conducting media audits and finding out from their core target how they use digital tools and what might be of value to them. Putting some effort and resources into understanding the myriad of different ways digital can be used, and physician preferences in this regard is relatively simple and will almost certainly have a payoff within a five-year timeframe. There will likely be some resistance from the sales folks who tend to see alternatives to face-to-face engagements as a threat to their position. However, I believe that the 21st century sales rep needs to be an expert in offline and online relationship building. Pharmaceutical companies need to figure out how to integrate different forms of digital and non-digital engagement optimally, and create internal structures and tools to maximize value for the customer.

McKinsey & Company article source:
Image sources:
‘Digital health collage’: Made the image myself
‘The alchemist’: https://openclipart.org/detail/222415/alchemist
‘Tools’: DeWalt DEWALT DWMT72163 118PC MECHANICS TOOL SET on http://toolguyd.com/dewalt-ratchets-sockets-mechanics-tool-sets/
‘Cartoon’: I’ve seen this cartoon on the web many times, but don’t know who made it originally. I’ve copied it from https://effectivesoftwaredesign.files.wordpress.com/2015/12/wheel.png?w=640
Since I started my business in healthcare-focused market research, I have been paying attention to wearable devices. Wearables devices have great potential for monitoring health parameters and improving care for certain chronic conditions.
The business press has been making a big deal of wearable devices, predicting exponential market growth over the next few years.
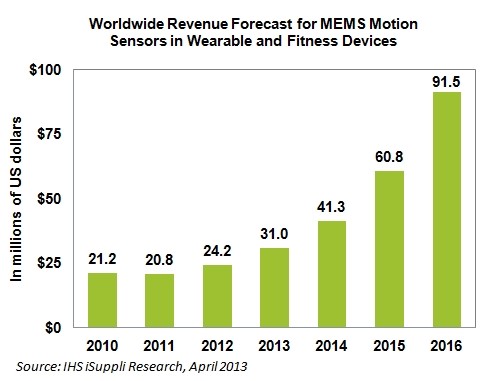
I am interested in the user perspective – how useful are these devices, actually? Some statistics show that, similar to fitness club memberships, many people who purchase fitness tracking wrist bands abandon them after a few months of usage.
As an anthropologist, I believe the best way to learn about a certain area of life is to immerse yourself in it, to experience what it feels like and to understand how it works. So I started going to these meet-ups for people engaged in the world of wearable devices. They are awesome!
Run in Steve-Jobs-style corporate presentations by the inspiring wearables guru Tom Emrich, companies in the wearables space present their prototypes and the audience gets to try stuff out in the post-presentation mix-and-mingle. My favorite so far has been the mind-controlled beer tap.
I have met many people in the wearables community, and they are certainly very different in style and outlook to my usual clientele (executives from pharma companies). However, I have hesitated to take the plunge into trying a wearable myself.
I am a pretty fit person, working out two to three times a week, to maintain my health and my sanity, eating pretty healthy, and most of the time walking to public transit rather than taking the car. Whether I run 5 minutes less today than I did last week is not really important to me, as long as I get some exercise every few days. Competing with others along fitness goals does not interest me at all. But I realized that not trying out a wearable myself would deprive me of certain insights that could be essential for conducting the user research that I am so interested in doing.
So I bought a Garmin Vivofit last week. Three things enticed me to purchase this device rather than some of the other ones that are very popular (Jawbone Up, Fitbit, Fuelband).

Here are my first experiences with the device:
Anyway, it has been a very interesting experiment so far, and definitely proof of the value of ‘walking in the shoes of’ to really understand something.
The true potential of wearables is difficult to tell at the moment. There could be all sorts of useful applications that have not yet been developed or that have not yet gained broad acceptance. After a lot of enthusiasm in the media, there seems to be a bit of a backlash now.
Here’s a recent page from The Atlantic, with quotes of tech opinion leaders all questioning the enthusiasm for wearables:

And here’s an article written by a health IT consultant about the more technical challenges of integrating mobile health monitoring devices into electronic medical records.
http://medicalconnectivity.com/2014/11/04/challenges-using-patient-generated-data-for-patient-care/
While I share some of the skepticism, the wearables space is certainly an area worth watching, and with great growth opportunities for companies who ‘get it right’. I am excited to be part of this journey.
Recently, the CBC reported on a ten-year old girl, Makayla Sault, who was diagnosed with acute lymphoblastic leukemia, a cancer of the blood. The girl experienced severe side effects from the chemotherapy she was receiving and decided, together with her parents, to discontinue therapy.
Now, the Children’s Aid Society is getting involved with the intent of convincing the family to complete the course of therapy. The parents and the community they live in also fear that Makayla may be forcibly removed from home and given therapy against her will.
Do parents have the right to choose whether or not a potentially life-saving treatment is given to their child? Does the child have a say in this decision? Does the state have the responsibility to act in what is perceived as the best interest of the child, against the parents’ and the child’s wishes?
Let’s consider all the factors.
Deadliness of the disease. The form of leukemia that Makayla has can progress very rapidly and lead to death within a few months, if not treated. If it was a slower progressing disease, would it seem reasonable to let the parents decide on the course of treatment?
Chance of cure. If treated, there is a high chance of long-term remission or cure for a patient with acute lymphoblastic leukemia. Some quote the likelihood of treatment success as 75% or even higher. How does this information influence your view on the case? Does the parents’ decision seem responsible? Should the state step in?
What if treatment success was estimated at 50%? …at 30%? …at 10%? How would this influence your view on whose right it is to decide what to do? With a low chance of remission or cure, would it seem reasonable to allow parents to, basically, let their child die without having to go through the agony of chemotherapy?
Cultural context. The news coverage focused in on the point that Makayla and her parents belong to the New Credit First Nation, based in Ontario. Her family decided to try traditional remedies instead chemotherapy, and their local community has shown great support for their decision. The interference of the Children’s Aid Society is seen by some as another attempt of a government agency to take away native children, as had been done during the era of forced residential schooling.
How does the cultural factor influence your view on the case? Does being First Nation give Makayla’s parents more of a right to decide her destiny than being of Irish decent, being Jewish or being Iranian? What if the family belonged to a religious group that was viewed as being ‘extremist’? Would you feel the same about the case or different?
To what extent is the state responsible for the well-being of our children, and to ensure their well-being in the face of parental opposition? Laws and mechanisms to protect children against abusive parents certainly seem appropriate. How about protecting children against well-meaning but ill-informed parents? How about protecting children against well-meaning, well-informed parents who adhere to a different belief system? Difficult decisions.
My friend had breast cancer twenty years ago. After surgery and radiation, she has been in remission and free of health complaints. Now that she is almost 80 years old, another lump was found in the same breast. She has access to excellent medical care, and she was given the following advice:
While the lump was small, she should have a mastectomy, just in case. As she was not eligible for another round of radiation therapy, it was recommended that she go through chemotherapy, because physiologically, she was deemed to be perhaps ten years younger than her actual age.
This is typical advice to elderly adults who are in good physical shape. It is based on the assumption that adding years to your life trumps every other consideration, provided you are in good health otherwise.
At age 80, how long does the average person have to live? Two years, five years, ten years tops? With all advances in medicine, we have not managed to extend life much beyond that. We are getting more and more people to reach their eighties, but we are not living significantly longer than that.
My friend was struggling with the advice she was given, and what was presented to her as the best medical solution. She did not want to lose her breast, and she did not want to put up with the side effects of chemotherapy. So she tried hard to find second and third opinions to support the view that it was not absolutely necessary to conduct a mastectomy and chemotherapy, and that she was not carelessly jeopardizing her chances of survival by refusing these options.
As we spoke about the different considerations that come into play in these decisions, she kept saying “I will get chemotherapy if I have to, but I’d rather not”. To me, this indicated an obligation that she felt to justify her choices to her friends and family, and perhaps to her medical advisors. Nobody wants to be seen as reckless with regard to one’s own health.
However, isn’t that bizarre and plain wrong? A person’s life is a person’s life, and having a lump in your breast is just one of many things you will consider and care about. So a woman who has carried two breasts through her entire life wants her life to end with both of them in place. So a woman who may have five, six or seven more years to live, probably deteriorating progressively as she ages, does not want to ruin her sense of well-being right now with an aggressive therapy regimen. So what?
Why is she made to feel guilty or irresponsible? Why does she need to justify her course of action?
It is understandable that friends and family of a person in this situation may advocate the more aggressive therapy, as they may fear losing this person. Fair enough.
However, it is my view that medical professionals should state very clearly that the choice is entirely up to the patient, that every choice has its trade-offs and that an informed choice, whatever it is, represents a responsible and acceptable way of managing one’s health. To have this sort of back-up from the medical community would make dealing with a difficult situation easier for the patient.
Taking breaks from your regular activity supposedly enhances your ability to concentrate. Consequently, the clever employer should encourage those who spend their day in front of the computer screen to interrupt their activity from time to time to relax and recharge.
I have a small beach ball in my office, a promotional item left over from some conference. What if I’d throw it up into the air? Today I tried it out: very relaxing – beats walking to the washroom or getting another cup of coffee. But I felt odd. What would my co-workers think about me? Sure looks like I’m goofing off.
In an office environment, some forms of de-stressing are more accepted that others. Getting coffee is the top accepted de-stresser, I would say. Smoking also features high on the list – need a break, have a smoke. Going for a walk – good, but may take too long in the eyes of the boss.
Many also deal with stress by talking to their fellow employees. Probably better for your health than smoking, but can cause significant disruption of the workflow, particularly if many employees go through a stressful time at once.
Spending five minutes with a beach ball (or a skipping rope? or a mini-putt?) seems like a worthwhile alternative that should be an acceptable form of recharging – and easier to monitor than other common forms of in-office relaxation, such as constantly checking your Twitter feed or Facebook updates. Then, I think, you are basically just goofing off…
Pharmaceutical companies have reoriented their businesses over the past several years to focus on discovery of molecules that target narrow markets, usually in oncology or in rare, but serious diseases. It is well known that revenues for ‘mass market’ products for diseases that are highly prevalent and not immediately life-threatening have been declining and few truly breakthrough discoveries have been made to replace revenue drivers that have become generic.
But why the rush into oncology and other small-but-serious markets? I believe that this has to do largely with our attitude towards death. Inevitably, we will all die of something. Before the advent of penicillin, people died of infections. As medical care has improved dramatically in the past 100 years, at least in some parts of the world, we live longer and are more likely to experience diseases which are basically a function of our body breaking down i.e. cancer.
Oncology drugs present an attempt to prevent the inevitable. In some tumour types, enormous advances have been made – breast cancer, for example, can now be regarded more as a chronic disease than as a terminal illness. For many other tumour types, however, scientific progress has been underwhelming. New agents are being trialed and approved that offer three or four more months of progression-free survival or a few months of overall survival vs. the incumbent standard of care. …and regulatory bodies such as the FDA find it difficult to turn those agents down, because they allow patients to live longer. Enormous costs to the healthcare system are perceived as justified, because they allow patients to live longer.
How much value do four extra months have when you are very sick and 80 years old? I don’t know, as I have not yet been in this situation. Who drives decisions to try another therapy, complete with side effects, at that point? Is it the physician, feeling compelled to offer a treatment when one is available? Is it the patient, clinging to life? Or is it the patient’s family, not wanting to let go?
One thing seems certain – no politician in his or her right mind will advocate spending healthcare dollars elsewhere, when there is time to be gained in the battle with death. Can you imagine the headlines? But the societal discourse may be shifting, looking at more humane ways of dealing with end-of-life, and re-evaluating our overall priorities in what kind of healthcare is being offered and funded.
Much has been published lately about personalized medicine. The other, similar buzzword is patient-centric.
It seems to me that in these terms, consultants and trend-spotters mesh together two very different ideas, each with associated with different strategic implications.
Personalized medicine in the sense of using biomarkers and genetic information to target therapies more specifically to patients who are more likely to respond to them is an approach that many pharmaceutical companies are embracing.
However, in this context the patient as a person has very little relevance for the R&D process and the commercialization of new products. What he or she feels, thinks, believes or does is unrelated to the peculiar genetic mutation that makes him or her a good candidate for a specific drug.
The second trend, namely focusing on the patient as a person, does not usually play a role in drug discovery. Pharmaceutical companies commonly find themselves in the situation that their compound is the third or fourth me-too agent to market with little incremental benefit. Identifying and targeting a specific patient with distinctive attitudes, behaviours and needs can be a successful marketing strategy in an undifferentiated market.
And while some companies may strive to bring both approaches closer together – understanding the patient as a person and developing new molecules that meet the patient’s specific needs – this is far more difficult to achieve in pharmaceutical product development than in the area of consumer goods.
Getting more exercise has undisputed health benefits. It is what many of us need. Experts also say that it makes you feel better. Why don’t more people get into the habit then?
In my experience, exercise does have a positive effect on mood – but not immediately. While exercising, anxiety, stress and frustration are felt even more acutely. That’s why, in my opinion, many people stay away from exercise. We don’t want to be brought face-to-face with unpleasant feelings.
However, to reap the benefits of a more relaxed mind, that’s exactly what we need to do. No pain, no gain. Good luck with the struggle!

{kind=link}